The cardiovascular system. Features of blood circulation in a human fetus: anatomy, scheme and description of hemodynamics What are the features of the fetal circulatory system
The fetal circulation occurs through the placenta, which receives 60% of the combined ventricular output, and after birth, most of it goes to the lungs.
Fetal circulatory system
When studying fetal circulation, several anatomical and physiological factors should be noted.
Normal adult circulation is represented by a series of circuits of blood flow through the right heart, lungs, left heart, systemic circulation, and back to the right heart. The fetal circulation is a parallel system with cardiac output from the right and left ventricles directed to different vessels. For example, the right ventricle, which provides about 65% of the combined output, pumps blood through the pulmonary artery, ductus arteriosus, and descending aorta. Only a small part of the emission from it passes through the pulmonary circulation. The left ventricle supplies blood mainly to tissues supplied by the aortic arch (for example, the brain). The fetal circulation is a parallel circuit characterized by channels (ductus venosus, foramen ovale, ductus arteriosus) that provide more highly oxygenated blood to the upper body and brain, less highly oxygenated blood to the lower half of the body, and low oxygenated blood to non-functioning lungs.
The umbilical vein, which carries oxygenated blood (oxygen saturation reaches 80%) from the placenta to the fetal body, enters the portal system. Part of the umbilical-portal blood passes through the microcirculation of the liver, where oxygen is released. From there, blood flows through the hepatic veins into the inferior vena cava. In the fetal circulation, most of the blood bypasses the liver through ductus venosus, directly penetrating the inferior vena cava, which also receives unsaturated (25%) venous blood from the lower half of the body. The blood that reaches the heart through the inferior vena cava is approximately 70% oxygenated (maximum highly oxygenated blood). About one third of the blood returning to the heart from the inferior vena cava flows predominantly through the right atrium, mixing with blood from the superior vena cava, then through the foramen ovale into the left atrium, where it mixes with a relatively small volume of venous blood from the lungs. Blood flows from the left atrium into the left ventricle, then into the ascending aorta.
From the proximal aorta, which carries the most oxygenated blood (65%) from the heart, branches depart for the blood supply to the brain and upper half of the body. Most of the blood returning through the inferior vena cava enters the right atrium, where it mixes with the unsaturated blood returned through the superior vena cava (25% oxygen saturation). Blood from the right ventricle (oxygen saturation - 55%) enters the aorta through the ductus arteriosus. The descending aorta supplies the lower half of the body with blood that is less oxygenated (about 60%) than the blood that comes to the brain and upper half of the body.
Of particular note is the role of the ductus arteriosus. Blood in the fetal circulation from the right ventricle enters the pulmonary trunk, from which, due to high vascular resistance, most of the blood bypasses the lungs through the ductus arteriosus and enters the descending aorta. Although the descending aorta gives off branches to the lower half of the fetal body, most of the blood from it flows to the umbilical arteries, which carry blood without oxygen to the placenta.
Oxygen exchange in the fetal circulation
Unlike the lungs, which need little oxygen, a statistically significant proportion of the oxygen obtained from the mother's blood during childbirth is consumed by the placental tissue. The degree of functional shunting of placental blood that has passed through the exchange centers is about ten times higher than in the lungs. The main reason for functional shunting is probably the mismatch between maternal and fetal blood flow in the exchange centers, which are examples of ventilation-perfusion inequalities similar to those in the lungs.
Uteroplacental circulation promotes gas exchange during fetal circulation. Oxygen, carbon dioxide and inert gases cross the placenta by simple diffusion. The degree of transfer is proportional to the difference in gas pressures and inversely proportional to the diffusion distance between maternal and fetal blood. The placenta does not serve as a significant barrier to the exchange of respiratory gases until it separates (placental abruption) or becomes edematous (severe fetal dropsy).
The figure shows the anatomical distribution of uterine and umbilical blood flow and oxygen transport across the placenta. The maternal shunt accounts for 20% of uterine blood flow and includes some of the blood diverted to the myoendometrium. The fetal shunt provides blood to the placenta and fetal membranes and accounts for 19% of umbilical blood flow. Maternal-fetal pressure gradients of oxygen and carbon dioxide are calculated in accordance with the parameters of gas tension in the uterine and umbilical arteries and vein. The fetal umbilical vein, like the adult pulmonary vein, carries the most oxygenated blood. The oxygen pressure in it is about 28 mm Hg, which is lower than in adults. Relatively low fetal voltage is required for intrauterine survival, as high oxygen pressure initiates physiological adaptations (eg, closure of the ductus arteriosus and pulmonary vasodilation) that normally occur in the neonate but adversely affect intrauterine life.
Not being involved in gas exchange, fetal respiratory movements are involved in lung development and respiratory regulation. Fetal respiration differs from adult respiration in that it is episodic in the fetus, sensitive to glucose concentration, and inhibited by hypoxia. Because of its sensitivity to acute oxygen deprivation, fetal respiration is used in clinical practice as an indicator of fetal oxygenation.
Curves of dissociation of hemoglobin in the fetus and mother
Most of the oxygen in the fetal circulation is carried by erythrocyte hemoglobin. The maximum amount of oxygen carried by 1 g of hemoglobin at 100% saturation is 1.37 ml. The volumetric rate of movement of hemoglobin depends on the degree of blood supply and the concentration of hemoglobin. Uterine blood flow by the end of pregnancy is 700-1200 ml / min, while about 75-88% of it falls on the intervillous space. The umbilical blood flow is 350-500 ml/min and more than 50% of the blood goes to the placenta.
The oxygen capacity of the blood is determined by the concentration of hemoglobin. It is expressed in milliliters of oxygen per 100 ml of blood. Closer to the end of pregnancy, the hemoglobin concentration in the fetus is about 180 g / l, and the oxygen capacity is 20-22 ml / dl. The oxygen capacity of the mother's blood, proportional to the concentration of hemoglobin, is lower than that of the fetus.
The affinity of hemoglobin for oxygen, expressed as a percentage of saturation at a given oxygen voltage, depends on chemical conditions. In the fetal circulation, hemoglobin oxygen binding under standard conditions (carbon dioxide pressure, pH, and temperature) is much higher than in non-pregnant adults. In contrast, the affinity of hemoglobin for oxygen in the mother under these conditions is lower: at a pressure of the latter of 26.5 mm Hg. (in the fetus - 20 mm Hg) 50% of hemoglobin is saturated with oxygen.
More heat fetal and lower in vivo pH shifts the oxygen dissociation curve to the right, while lower maternal temperature and higher pH shifts the curve to the left. As a result, oxygen dissociation curves for fetal and maternal blood do not differ as much at the placental junction. The maternal venous oxygen saturation is probably 73%, and its pressure is about 36 mm Hg. The corresponding values for blood from the umbilical vein are approximately 63% and 28 mmHg. As the only source of oxygen for the fetus, the umbilical vein blood has a higher oxygen saturation and pressure than the fetal blood. With low oxygen pressure in the arterial blood of the fetus, its oxygenation is supported by an increase in blood flow in the tissues caused by an increase in cardiac output. Along with a lower saturation of blood hemoglobin with oxygen, this leads to its normal supply to the fetal organs.
The decrease in the affinity of hemoglobin for oxygen caused by a decrease in pH is referred to as the Bohr effect. Due to the special situation in the placenta, the double Bohr effect facilitates the transfer of oxygen from the mother to the fetus. When there is transfer of carbon dioxide and associated acids from fetus to mother, the concomitant increase in fetal pH increases the affinity of fetal erythrocytes for oxygen uptake. The concomitant decrease in maternal blood pH reduces the affinity for oxygen and promotes the unloading of oxygen from her red blood cells.
Changes in the anatomy of the cardiovascular system after birth
After birth, there following changes fetal circulation and cardiovascular system.
- Termination of placental circulation with rupture and further obliteration of the umbilical vessels.
- Closure of the venous duct.
- Closure of the foramen ovale.
- Gradual narrowing and further obliteration of the arterial duct.
- Expansion of pulmonary vessels and formation of pulmonary circulation.
Termination of the umbilical circulation, closure of vascular shunts and formation of the pulmonary circulation lead to the fact that the newborn's circulatory system turns from parallel to the maternal one into a closed and completely independent one.
The article was prepared and edited by: surgeonIn the embryonic and fetal period in higher vertebrates, 3 circulatory systems are formed: yolk, placental and pulmonary.
In the initial stages of development, after the isolation of the umbilical vesicle, yolk circulation occurs, which consists in the appearance of arterial and venous vessels that braid the wall of the yolk sac and gather into larger trunks in the region of the umbilical ring. This circulatory system has great importance in oviparous. In mammals, it is poorly developed, it is formed almost simultaneously with the placental circulation.
The latter performs the functions of the pulmonary circulation of adult individuals, since the pulmonary circulation does not function in the embryo. Placental circulation is characterized by the following anatomical features: the left and right halves of the heart are not isolated, but are connected by an oval hole located between the atria, a membranous valve is attached to the edges of this hole, which is pressed into the cavity of the left atrium. The pulmonary artery is connected to the aorta by a large anastomosis, as a result of which the bulk of the blood from the right ventricle enters the aorta. A small amount of blood flows into non-functional lungs. Two umbilical arteries separate from the aorta, they go along the side walls Bladder, penetrate through the umbilical canal, participating in the formation of the umbilical cord. Located between the allantois and the chorion, the branches of the umbilical arteries approach the fetal part of the placenta and form a dense arterial network there, penetrating the end branches into each villus. Arterioles of the villi pass into venules, the latter, gathering into larger trunks, form the umbilical vein. The umbilical vein as part of the umbilical cord passes into the abdominal cavity and goes to the liver, where it flows into the portal vein. Ruminants and carnivores have an additional venous duct connecting the umbilical vein to the caudal vena cava. Features of the fetal circulation: fetal blood is always poorer in oxygen than the mother's blood, since oxygen is captured by fetal erythrocytes only in the villi of the placenta; the umbilical vein carries oxygenated blood; in the liver, the blood of the umbilical vein mixes with the venous blood of the portal vein; through the foramen ovale, blood from the right atrium enters the left atrium, mixes with venous blood from the pulmonary vein and enters the right ventricle; blood entering the right ventricle is distilled by its contraction from the pulmonary artery through the ductus arteriosus into the aorta. As a result of this mixing, the blood of a large circle contains little oxygen and the umbilical arteries carry "venous" blood.
During childbirth, when the umbilical cord is compressed or broken, the fetus reflexively inhales, at the same time as the foramen ovale valve closes, thus the right and left atrium are isolated. After birth, the provisional vessels of the fetus turn into ligaments.
The growth of the embryo and fetus is extremely fast, so it needs intensive nutrition. In many vertebrates, the fetus feeds on the yolk of the egg. In organisms at a higher stage of development, the nutrition of the fetus is partly due to the yolk of the cell, but mainly as a result of the plastic material of the maternal organism due to the placental connection between the heart and the mother. The higher the organization of the animal, the smaller the role in the nutrition of the embryo is played by the reserves of plastic material laid down in the egg cell. The circulatory systems of the mother and fetus are closely related.
In the first days, the embryo develops due to the reserves of the cytoplasm of the egg. This explains the fact that during intensive crushing in the morula stage, the size of the embryo does not change. After the disappearance of the transparent shell, it begins to grow rapidly, scooping plastic material from the mother's body. With the penetration of the embryo into the uterus, the trophoblast takes up nutrients from the embryotorf (“uterine milk”). Embryotorf is the secret of the uterine mucosa. Soon a network of blood vessels of the yolk circle of blood circulation develops, it extracts the nutrient material from the yolk sac and distributes it to all elements of the embryo. In domestic animals, the yolk circulation cannot provide the fetal need for nutrients, this role is played by the placental circulation. The placenta replaces for the fetus the activity of a number of organs involved in the metabolism of an adult animal. The functions of the placenta are carried out not only by osmosis and diffusion, but also through complex biochemical transformations of substances.
The paths of the primary, or yolk, blood circulation, represented in the fetus by the umbilical-mesenteric arteries and veins, are the earliest to form. This blood circulation for a person is rudimentary and has no significance in gas exchange between the mother's body and the fetus.
The main circulation of the fetus is chorionic, represented by the vessels of the umbilical cord. Chorionic (placental) circulation begins to provide fetal gas exchange from the end of the 3rd - the beginning of the 4th week of intrauterine development. The capillary network of chorionic villi of the placenta merges into the main trunk - the umbilical vein, which passes as part of the umbilical cord and carries oxygenated and nutrient-rich blood. In the body of the fetus, the umbilical vein goes to the liver and, before entering the liver, through a wide and short venous (arantian) duct gives a significant part of the blood into the inferior vena cava, and then connects to the relatively poorly developed portal vein. Thus, the liver receives maximally oxygenated blood from the umbilical vein already at some dilution with purely venous blood from the portal vein.
After passing through the liver, this blood enters the inferior vena cava through the system of recurrent hepatic veins. The mixed blood in the inferior vena cava enters the right atrium. Pure venous blood from the superior vena cava, flowing from the cranial regions of the body, also enters here. At the same time, the structure of this part of the fetal heart is such that there is no complete mixing of the two blood streams. Blood from the superior vena cava is sent mainly through the right venous opening to the right ventricle and pulmonary artery, where it bifurcates into two streams, one of which (smaller) passes through the lungs, and the other (larger) enters the aorta through the arterial ductus arteriosus and is distributed between the lower segments of the fetal body. Blood entering the right atrium from the inferior vena cava enters predominantly into the wide gaping foramen ovale and then into the left atrium, where it mixes with a small amount of venous blood that has passed through the lungs and enters the aorta to the confluence of the ductus arteriosus, thus providing better oxygenation and trophism of the brain, coronary vessels and the entire upper half of the body. The blood of the descending aorta, which has given up oxygen, returns through the umbilical arteries to the capillary network of the chorionic villi of the placenta. Thus, the circulatory system functions, which is vicious circle, isolated from the mother's circulatory system, and acting solely due to the contractility of the fetal heart. Certain assistance in the implementation of fetal hemodynamics is provided by respiratory movements starting from the 11-12th week. The periods of negative pressure that occur during them in the chest cavity with unexpanded lungs contribute to the flow of blood from the placenta to the right half of the heart. The viability of the fetus depends on the supply of oxygen and the removal of carbon dioxide through the placenta into the maternal circulation.
The umbilical vein carries oxygenated blood only to the inferior vena cava and portal vein. All organs of the fetus receive only mixed blood. However, the best oxygenation conditions are found in the liver, brain and upper extremities, the worst conditions are in the lungs and lower half of the body.
The degree of oxygen saturation of the umbilical vein blood changes during pregnancy. At 22 weeks it is 60%. In the future, when pregnancy is prolonged, saturation may decrease and drop to 30% at the 43rd week. The oxygen saturation of the blood of the umbilical arteries is 40% at the 22nd week, at 30-40th -25%, and by the 43rd week it drops to 7%. Despite the relatively low blood oxygen saturation, the arteriovenous difference in the fetus is about 20%, which approaches the arteriovenous difference in an adult (20 - 30%). The partial pressure of oxygen in the umbilical vein of the fetus is 21 - 29 mm Hg. Art., or 2.80 - 3.87 kPa, and in the umbilical artery - from 9 to 17 mm Hg. Art., or 1.20 - 2.27 kPa.
The partial pressure of carbon dioxide, respectively, is 42 - 45 mm Hg. Art., or 5.60 - 6.00 kPa, and 45 - 49 mm Hg. Art., or 6.00 - 6.53 kPa. The conditions of placental circulation and gas exchange ensure the normal physiological development of the fetus at all stages of pregnancy. Factors that significantly contribute to the adaptation of the fetus to these conditions are an increase in the respiratory surface of the placenta, an increase in blood flow velocity, an increase in the amount of hemoglobin and erythrocytes in the fetus, the presence of a particularly high oxygen-binding ability of fetal hemoglobin, as well as a significantly lower need for fetal tissues in oxygen. However, as the fetus grows and the gestational age increases, the conditions for gas exchange deteriorate significantly. The reason for this is probably the relative lag in the growth of the respiratory surface of the placenta.
The heart rate of the human embryo is relatively low (15 - 35 per minute). With the formation of placental circulation, it increases to 125-130 per minute. In the normal course of pregnancy, this rhythm is extremely stable, but in pathology it can sharply slow down or accelerate. This indicates the early maturation of reflex and humoral regulatory effects on the intrauterine circulatory system. The sympathetic and somewhat later parasympathetic innervation of the heart matures earlier. The blood circulation of the fetus is the most important mechanism of its life support, and therefore control over the activity of the heart is of the most direct practical importance in monitoring the course of pregnancy.
text_fields
text_fields
arrow_upward
The fetus receives the nutrients and oxygen necessary for life from the mother through the vessels. children's place, or placenta.
The placenta is connected to the fetus by the umbilical cord, which contains two umbilical arteries(branches of the internal iliac arteries of the fetus) and umbilical vein. These vessels pass from the cord into the fetus through an opening in its anterior abdominal wall (umbilical ring). Through the arteries, venous blood is delivered from the fetus to the placenta, where it is enriched with nutrients, oxygen and becomes arterial. After that, the blood returns to the fetus through the umbilical vein, which approaches his liver and divides into two branches. One of them flows directly into the inferior vena cava (ductus venosus). Another branch passes into the gates of the liver and divides into capillaries in its tissue.
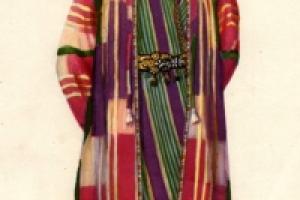
Rice. 2.17 Fetal circulation
From here, blood flows through the hepatic veins into the inferior vena cava, where it mixes with venous blood from the lower body and enters the right atrium. The opening of the inferior vena cava is located opposite the oval opening in the interatrial septum (Fig. 2.17). Therefore, most of the blood from the inferior vena cava enters the left atrium, and from there into the left ventricle. In addition, the pulsatile flow of blood from the placenta through the umbilical vein can temporarily block the flow of blood through the portal vein. Under these conditions, predominantly oxygenated blood will enter the heart. In the intervals, venous blood enters the heart through the superior and inferior vena cava.
As described earlier, most of the venous blood from the right atrium enters the right ventricle, and then into the pulmonary artery. A small amount of blood goes to the lungs, but most of it enters the descending aorta through the arterial duct after the arteries leave it to the head and upper limbs and diverges through the systemic circulation connected through the umbilical arteries to the placenta.
Thus, both ventricles pump blood into the systemic circulation, so their walls are almost equal in thickness. Purely arterial blood flows in the fetus only in the umbilical vein and ductus venosus. All other fetal vessels circulate mixed blood, but the head and upper body, especially in the first half of fetal development, receive blood from the inferior vena cava, less mixed than the rest of the body. This contributes to a better and more intensive development of the brain.
Circulatory changes after birth
text_fields
text_fields
arrow_upward
At birth, the placental circulation is interrupted and pulmonary respiration is switched on. Enrichment of blood with oxygen occurs in the lungs. Clamping of the umbilical vessels leads to a decrease in the amount of oxygen and an increase in the amount of carbon dioxide in the circulating blood. Irritation of receptors in the walls of blood vessels and neurons of the respiratory center causes a reflex inhalation. With the first breath of a newborn, the lungs expand and all the blood from the right half of the heart passes through the pulmonary artery into the pulmonary circulation, bypassing the ductus arteriosus and foramen ovale. As a result, the duct becomes empty, the smooth muscle cells in its wall contract and after some time overgrow, remaining in the form of an arterial ligament. The foramen ovale is obscured by the fold of the endocardium, which soon grows to its edges, causing the hole to turn into an oval fossa.
From birth, venous blood circulates in the right half of the heart, and only arterial blood circulates in the left. The vessels of the umbilical cord become empty, the umbilical vein turns into a round ligament of the liver, the umbilical arteries - into the lateral umbilical ligaments that run along the inner surface of the abdominal wall to the navel.
Age-related changes in the structure of the circulatory system
text_fields
text_fields
arrow_upward
The heart of children of the first year of life is spherical, the walls of the ventricles differ little in thickness. The atria are large, while the right is larger than the left. The mouths of the vessels flowing into them are wide. In the fetus and newborn, the heart is located almost across the chest. Only by the end of the first year of life, due to the transition of the child to a vertical position of the body and the lowering of the diaphragm, the heart takes an oblique position. In the first two years, the heart grows vigorously, and the right ventricle lags behind the left. An increase in the volume of the ventricles leads to a relative decrease in the size of the atria and their ears. From 7 to 12 years of age, the growth of the heart is slow and lags behind the growth of the body. During this period, careful medical monitoring of the development of schoolchildren is especially important, aimed at preventing heart overload (hard physical work, excessive sports, etc.). During puberty (at 14-15 years old), the heart grows rapidly again.
The development of blood vessels is associated with the growth of the body and with the formation of organs. For example, the more intensively the muscles function, the faster the diameter of their arteries increases. The walls of large arteries form faster, with the most noticeable increase in the number of layers of elastic tissue in them. This stabilizes the propagation of the pulse wave through the arterial vessels. In children, more intense than in adults, blood flow is observed in the brain. Blood flow changes little during exercise, these changes are different in children different ages. Using the rheoencephalography method, it was found that in right-handed people during exercise, the blood flow in the left hemisphere increases more intensively than in the right one.
Slow heart enlargement continues after 30 years. Individual fluctuations in the size and weight of the heart may be due to the nature of the profession. By old age, the number of elastic and muscular elements in the walls of the aorta and other large arteries and veins decreases, connective tissue grows, the inner membrane thickens, and seals form in it - atherosclerotic plaques. As a result, the elasticity of the vessels decreases markedly, and the blood supply to the tissues deteriorates.
This article is the first part of a cycle about the heart and blood circulation. Today's material is useful not only for general development, but also for understanding what heart defects are. For better presentation posted a lot of drawings, and half with animation.
Scheme of blood flow in the heart AFTER birth
Deoxygenated blood from the whole organism is collected in the right atrium along the superior and inferior vena cava (along the upper - from the upper half of the body, along the lower - from the lower). From the right atrium, venous blood enters the right ventricle through the tricuspid valve, from where it enters the lungs through the pulmonary trunk (= pulmonary artery).
Scheme: hollow veins? right atrium? ? right ventricle? [pulmonary valve] ? pulmonary artery.
The structure of the adult heart(picture from www.ebio.ru).
arterial blood from the lungs along 4 pulmonary veins (2 from each lung) is collected in the left atrium, from where through the bicuspid ( mitral) valve enters the left ventricle, and then through the aortic valve is ejected into the aorta.
Scheme: pulmonary veins? left atrium? [mitral valve] ? left ventricle? [aortic valve] ? aorta.
Scheme of the movement of blood in the heart after birth(animation).
Superior vena cava - superior vena cava.
Right atrium - right atrium.
Inferior vena cava - inferior vena cava.
Right ventricle - right ventricle.
Left ventricle - left ventricle.
Left atrium - left atrium.
Pulmonary artery - pulmonary artery.
Ductus arteriosus - arterial duct.
Pulmonary vein - pulmonary vein.
Diagram of blood flow in the heart BEFORE birth
In adults, everything is simple - after birth, the blood streams are separated from each other and do not mix. In the fetus, blood circulation is much more difficult, which is associated with the presence of the placenta, non-working lungs and the gastrointestinal tract. The fetus has 3 features:
- open oval hole(foramen ovale, "foramen ovale"),
- open ductus arteriosus(botall duct, ductus arteriosus, "ductus arteriosus")
- and open ductus venosus(ductus venosus, "ductus venozus").
The foramen ovale connects the right and left atrium, the arterial duct connects the pulmonary artery and the aorta, and the venous duct connects the umbilical vein and the inferior vena cava.
Consider the flow of blood in the fetus.
Diagram of the fetal circulation
(explanations in the text).
Oxygen-enriched arterial blood from the placenta through the umbilical vein, passing in the umbilical cord, enters the liver. Before entering the liver, the blood flow is divided, and a significant part of it bypasses the liver through ductus venosus, which is present only in the fetus, and goes into the inferior vena cava directly to the heart. Blood from the liver itself through the hepatic veins also enters the inferior vena cava. Thus, before flowing into the right atrium in the inferior vena cava, mixed (venous-arterial) blood is obtained from the lower half of the body and the placenta.
Through the inferior vena cava, mixed blood enters the right atrium, from where 2/3 of the blood through the open oval hole enter the left atrium, left ventricle, aorta and systemic circulation.
oval hole and ductus arteriosus at the fetus.
Movement of blood through the foramen ovale(animation).
The movement of blood through the ductus arteriosus(animation).
1/3 of the mixed blood received through the inferior vena cava is mixed with all purely venous blood from the superior vena cava, which collects blood from the upper half of the fetal body. Further from the right atrium, this flow is directed to the right ventricle and then to the pulmonary artery. But the lungs of the fetus do not work, so only 10% of this blood enters the lungs, and the remaining 90% through arterial (botallian) duct are discharged (shunted) into the aorta, worsening oxygen saturation in it. From the abdominal part of the aorta, 2 umbilical arteries depart, which in the umbilical cord go to the placenta for gas exchange, and begins new circle circulation.
Liver The fetus is the only one of all organs that receives pure arterial blood from the umbilical vein. Thanks to the “preferential” blood supply and nutrition, by the time of birth, the liver has time to grow to such an extent that it takes 2/3 abdominal cavity and in relative terms weighs 1.5-2 times more than an adult.
Arteries to the head and upper body depart from the aorta above the level of the confluence of the ductus arteriosus, so the blood flowing to the head is better oxygenated than, for example, the blood flowing to the legs. Like the liver, the newborn's head is also unusually large and occupies 1/4 of the entire body length(in an adult - 1/7). Brain newborn is 12 - 13% of body weight(in adults 2.5%). Probably, small children should be extraordinarily smart, but we cannot guess this because of the 5-fold decrease in brain mass. 😉
Circulatory changes after birth
When a newborn takes its first breath, it lungs expand, vascular resistance in them drops sharply, and blood begins to flow into the lungs instead of the arterial duct, which first empties and then overgrows (scientifically speaking, obliterated).
After the first breath, the pressure in the left atrium increases due to increased blood flow, and foramen ovale ceases to function and grows. The venous duct, the umbilical vein and the terminal sections of the umbilical arteries also overgrow. Blood circulation becomes the same as in adults.
Heart defects
Congenital
Since the development of the heart is quite complex, this process can be disrupted during pregnancy by smoking, drinking alcohol, or certain medications. Congenital heart defects are in 1% of newborns. Most often registered:
- defect(non-closure) of the interatrial or interventricular septum: 15-20%,
- wrong location ( transposition) aorta and pulmonary trunk - 10-15%,
- Fallot's tetrad- 8-13% (narrowing of the pulmonary artery + malposition of the aorta + ventricular septal defect + right ventricular enlargement),
- coarctation(narrowing) of the aorta - 7.5%
- open ductus arteriosus - 7 %.
Acquired
Acquired heart defects occur in 80% of cases due to rheumatism(as they say now, acute rheumatic fever). Acute rheumatic fever occurs 2 to 5 weeks after a streptococcal throat infection ( angina, pharyngitis). Since streptococci are similar in their antigenic composition to the body's own cells, the resulting antibodies trigger damage and inflammation in the circulatory system, which ultimately leads to the formation of heart defects. The mitral valve is affected in 50% of cases.(if you remember, it is also called bicuspid and is located between the left atrium and ventricle).
Acquired heart defects are:
- isolated (2 main types):
- valve stenosis(narrowing of the lumen)
- valve insufficiency(incomplete closure, resulting in reversed blood flow during contraction)
- combined (stenosis and insufficiency of one valve),
- combined (any defeat of different valves).
It is worth noting that sometimes combined defects are called combined, and vice versa, because. there are no clear definitions here.